


Firefighting 3.0
Using data, common sense and thinking differently can transform the fire service. First in a series

In my Thanksgiving post on gratitude, No. 1 on my list was my health. I referenced a book I had recently read by Dr. Peter Attia, Outlive, The Science and Art of Longevity. Broadly speaking, the book argues that healthcare needs to transition from what Dr. Attia calls Medicine 2.0 to a new and much-improved Medicine 3.0.
We’ve become astoundingly good at treating folks who are really sick or badly injured — that’s Medicine 2.0. Obviously, it’s not a bad thing that we’ve made such amazing advances in modern medicine. I think of my sister’s recovery from Stage 4 ovarian cancer to pretty much cancer free in less than 12 months. It’s a wonderful, glorious thing. In fact, it was about this time two years ago she called Beloved Wife and I to break the bad news: she had a large growth in her belly along with significant fluid buildup in her abdomen. When I went to visit her in Houston after the call, I did my best to hide my shock when I saw her. Her face was drawn, she had lost a lot of weight and had trouble walking up the stairs in her home. “She’s dying,” I thought.
Indeed, without Medicine 2.0 there’s no doubt in my mind she would have passed away within months if not for the aggressive chemotherapy, followed by surgery to remove a cancerous mass on her ovaries as well as some spots on her liver, followed by more chemotherapy. To look at her now, you’d never know she was sick a day in her life. To me, what medical professionals can do for us these days is nothing short of miraculous.
Yet …
Dr. Attia believes we could and should be doing much better. I’ll let him describe the four primary differences between Medicine 2.0 and Medicine 3.0.
Medicine 3.0 places a far greater emphasis on prevention than treatment. When did Noah build the ark? Long before it began to rain. Medicine 2.0 tries to figure out how to get dry after it starts raining. Medicine 3.0 studies meteorology and tries to determine whether we need to build a better roof, or a boat.
Second, Medicine 3.0 considers the patient as a unique individual. Medicine 2.0 treats everyone basically the same, obeying the findings of the clinical trials that underlie evidence-based medicine. … The problem is no patient is strictly average. Medicine 3.0 takes the findings of evidence-based medicine and goes one step further, looking more deeply into the data to determine how our patient is similar or different from the “average” subject in the study and how its findings might or might not be applicable to them. Think of it as “evidence-informed” medicine.
The third philosophical shift has to do with our attitude toward risk. In Medicine 3.0, our starting point is the honest assessment, and acceptance, of risk — including the risk of doing nothing.
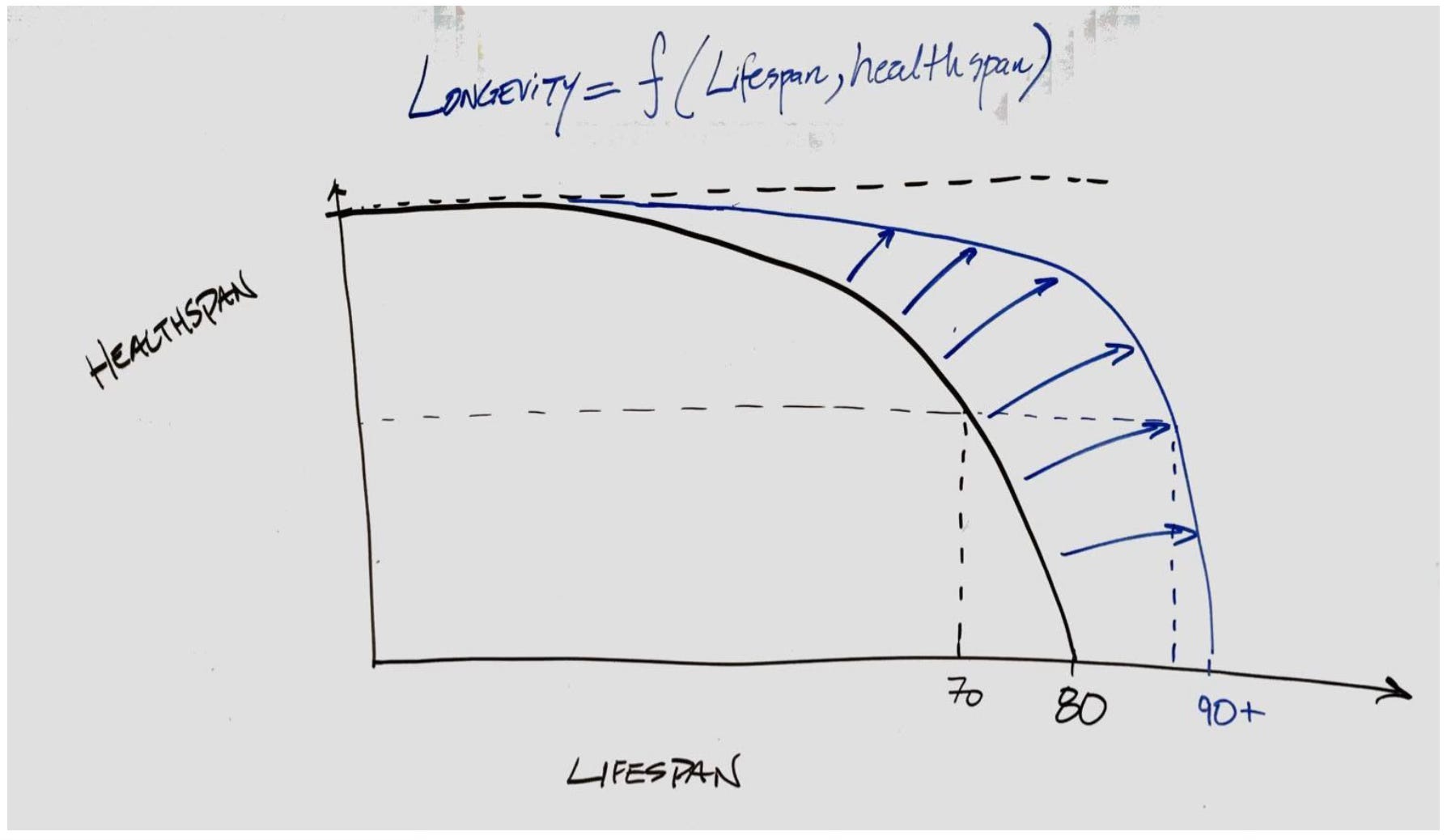
The fourth and perhaps largest shift is that where Medicine 2.0 focuses largely on lifespan, and is almost entirely geared toward staving off death, Medicine 3.0 pays far more attention to maintaining healthspan, the quality of life.
Healthspan is about maintaining our physical and cognitive capacities. When our bodies decline, we lose muscle mass and strength, along with bone density, stamina, stability and balance. When our minds decline, processing speeds slow down, we can’t solve complex problems like we used to, and memory fades.
Here’s a chart Dr. Attia drew on his office whiteboard to explain optimal longevity to one of his patients.
Robert Isbell wants to change firefighting in the same way. Not the actual fighting of fires — that’s actually a very small component of what firefighters do these days — but in how firefighters take care of their communities. In short, he’d like to reduce the frequency of emergency 9-1-1 calls in much the same way Dr. Attia wants to prevent folks from having a miserable last 10 years of their lives as their minds and bodies decline in ways that are mostly preventable.
Isbell has spent his 30-plus year fire service career in Texas, serving as Fire Chief in the cities of Southlake, Euless, Midland, Round Rock and currently in Stephenville. I got to know him when he was in Round Rock — which happened to coincide with the COVID pandemic. He always had the latest medical information on the disease, and really helped keep City employees on an even keel, especially during the early days of the pandemic when there were so many unknowns. He’s an avid reader — I knew before I asked him if he had read Dr. Attia’s book (of course he had. And then he recommended two books to me before we finished our interview last week).

He was a perfect fit for Round Rock — whip smart, progressive, proactive and easy to work with. He started the Community Risk Reduction program, which is basically Firefighting 3.0. It’s a radical departure from traditional firefighting, but once you learn about it — just like with Dr. Attia’s Medicine 3.0 — you wonder why the hell everyone’s not doing business this way. Have a look.
For readers not familiar with the fire service, let me share a fact that might surprise you. The U.S. Fire Administration reports only 4 percent of all reported fire department runs were fire related. Nearly two-thirds (64 percent) of the reported calls required emergency medical services (EMS) and rescue services from fire departments.
Frankly, I wonder why we still call them firefighters. Don’t get me wrong — they do still fight fires and God bless them for the courage to do that. It’s a dangerous business, no doubt. But as the statistics show, putting the wet stuff on the hot stuff is not how they spend most of their time.
Isbell said the majority of the EMS runs his team makes in Stephenville are what he calls low acuity. He says about 15-20 percent are actual emergencies, i.e., someone needs to get to the hospital ASAP.
But those low-acuity calls aren’t a waste of time. At least, not for a guy like Chief Isbell.
“We see these cases where people live … differently,” Isbell says, pausing to find the right word. “And there’s not a politically correct way to say it, but they’re living below a standard.”
There could be mental health issues, or environmental issues, or a combination of both — as is the case with hoarders. Maybe they’ve run out of their medicine, or it’s not working anymore. They’re having problems, just not the kind that require an ambulance transport to the emergency room.
“We go out and we see these people, we run a call, we take care of an issue, we see it, and then we walk away from it,” Isbell says. “And in my past, we all just kind of looked the other way. And it gets to weighing on you the more you see some of these conditions that people live in, and you say to yourself, ‘That shouldn’t be, and I know about it. Shouldn’t I tell somebody or do something?’”
The turning point for Isbell came on a call in Midland, which sits in the heart of the West Texas oil patch and where he worked from 2010 to 2016.
“We had a fire death,” he said. “It was in the winter, and we had a young man that was living in a garage, kind of a boarded-up garage, behind a house. And when I got there, the battalion chief met me in the yard, and he was distraught. He grabs me and says, ‘This shouldn’t have happened. This shouldn’t have happened.’ And I grabbed him thinking, I need to console him and say, ‘Yes, I know, it’s terrible.’ He says, ‘No, you don’t understand. We knew that he lived here like this. We should have done something before today to make sure this didn’t happen.’
“And I’ll tell you, that hit me right between the eyes like a hammer, thinking, what are we doing?”
Isbell wasn’t the only fire chief asking that question. He connected with Assistant Chief Norman Seals in Dallas and Chief Danny Kistner in McKinney, Texas, (both have since retired) to talk about “how to attack this problem of low-acuity EMS calls in a population that needed help that wasn’t exactly getting it, and whether we (in the fire service) could be the vehicle for it,” Isbell said.
More fire service agencies nationwide are taking this thoughtful approach to serving the public. Over the past decade, local healthcare gaps have been filled through Community Paramedic programs that use EMS personnel to fill gaps in the healthcare system, particularly in management of non-acute illnesses, mental health issues and chronic care follow-up needs. EMTs can now earn a certification in Community Paramedicine.
Other than running reports to identify “frequent flyers,” i.e., those folks who continually call 9-1-1 for low acuity care, how do firefighters find those in need? Here’s where the story gets really interesting, and Isbell’s creativity shines through.
When reading The Power of Habit: Why We Do What We Do in Life and Business, by Charles Duhigg, Isbell was struck by how Target uses data analytics to send targeted mailers to people based on their demographic profile and by analyzing what they had recently purchased.
“They could tell if a woman was pregnant based on her purchases, whether she knew it or not,” Isbell says. “And (Duhigg) told a story about how they would send targeted ads for baby stuff (based on) these specific purchases that women were making. And they got a call one day from angry dad of a 16-year-old girl who said, ‘Look, you’re sending my daughter all of this baby stuff. Cut it out. She’s 16 years old. I don’t know what you’re doing.’ And Target says, ‘Hey, look, we’re sorry. We follow a model … We’re sorry. We’ll stop.’ And a few weeks later, the dad calls back to say, hey, sorry, you were right, she was pregnant.”
So, Isbell thinks, if a Target store can tell if a woman is pregnant based on her shopping habits, surely a fire department can use data analytics to predict where their next fire is going to be. He says he actually called Target HQ to see if they could help him analyze data.
“They graciously declined,” he says with a laugh.
But he convinced his City Manager to buy consumer data so they could dig into it in order to identify high risk properties. They added data from other sources — like home sale information — to further refine their targeting efforts.
“We tried to find markers that I believed would be indicative of a fire risk,” Isbell said. “Stuff like age, education, income, that sort of thing, but we layered in data like the age of a house. But it wasn’t just that it was an old house, but how long (the same family) had lived in a house. The longer you live in a house, the more suspect it becomes of risk. So, if it’s a 100-year-old house and had been sold five years ago … then I knew that it had been inspected at least when they got a new mortgage on it. But if it’s a 100-year-old house and they’d been in it for 80 years, that’s a risky house.”
Using the data, they selected 1,000 homes for smoke detector inspections and installations. While getting smoke detectors in homes is good in and of itself, it’s also an opportunity to look for potential fire hazards. The Midland FD assembled a small army of volunteers who put door hangers on 1,000 doors, letting the residents know they’d be back in a week for the smoke detector inspections.
Bingo!
“The night we did the door hangers, we had a fire in one of the houses, burned the house up,” Isbell said. “It was late night. I remember I rushed across town because I got a call saying, ‘Hey, one of the houses caught fire that we put a door hanger on.’ Well, I was just crazy excited thinking, ‘I’m right. My data is right. Oh my gosh.’ But they had a fire. Are we too late?”
The good news was, they weren’t. Everyone got out of the house safely. Talking with the homeowners, Isbell said he wished the department volunteers been out placing door hangers a week earlier.
“And they said, ‘Oh, yeah, we saw it. We saw your flyer today. We went and checked our smoke detectors because we saw your flyer, and that’s what alerted us to get out.’ So in one way, I wanted to high five myself in the yard. But on the other hand, I’m thinking, but what would I have found if I would have been in there?”
What they would have found, Isbell said, was a box fan that ran continuously in a room where the family kept pets. The motor got dirty and caught fire. Which led to another prevention protocol.
“Every community does box fan giveaways during the summer,” he said. “We were giving away fans to the elderly at that time. I couldn't sleep that night. I went to work, and I looked up box fan fires, and it scared me. Box fans catch fire a lot, OK? They need to be properly cared for; they’re not made to run 24-7, and they have to be clean. I immediately drew up a one-page information flyer for box fans … and I made sure that there was a stack of those flyers on those box fans. And nobody got a box fan without one of those information flyers. And now that’s a part of our home safety inspection.”
The inspections also include checking behind stoves, pulling them away from walls and sweeping behind them. (“They’re all embarrassed. But everybody’s got junk behind their stoves.”) They’re making sure the gas or electrical connections are in good shape.
“The No. 1 cause of fires in America, in every community, is cooking fires,” Isbell said. “So we want to make sure that area is safe.”
They’ll also look for black smoke marks around electrical outlets. In Midland, a bunch of electricians volunteered to replace the suspect ones.
“We’ve got electricians that volunteer. It’s not taxpayer money,” Isbell says. “They come in, they install them for free. Now, my most vulnerable demographic is a little bit safer” because they’ve got functioning smoke detectors, a tidied-up cooking area, safe electrical outlets and clean box fans.
Those home inspections have become more than fire prevention programs; they’re an opportunity for a kind of well care check for residents in need. During those inspections, “we develop a relationship with them, find out a little more about them,” Isbell says.
“If we’ve never run an ambulance call on them, I really want to know a little more,” Isbell says.
So they’ll ask, “How are you doing? How’s your health? Are you taking medications on a regular basis?”
“It’s amazing what people will tell a fireman,” Isbell says. “They’ll sit down and tell us their life story.”
Next week, we’ll go deeper into Firefighting 3.0 and talk to a firefighter on the front lines who’s hearing those life stories.
Onward and Upward.
Will,
This is music to my ears.
What a powerful story of great leadership!
Robert Isbell is a man on a mission.
This is truly what it takes to change the world.
He is DOING it.
Prevention IS The Solution.
It is the solution on all levels of life.
Through insight and effective targeted action,
most of the problems that cause suffering and destruction
CAN be prevented.
You have shared these powerful ideas with us here
and given us a deeply inspiring example.
A loving servant leader in ACTION
tending his flock.
As for the world,
the move from 2.0 to 3.0 in all fields
is our next revolution.
A wonderful, liberating and life-giving revolution
just as important as the victory of democracy.
To reach level 3.0 we must always seek
to address the CAUSE of the problem,
as you have been doing all along in your essays here,
for that is the only path to long term prevention.
To offer an illustration from the field of psychology:
until we understand the CAUSE of school shootings
we will be unable to prevent them.
Yes, we can REDUCE them via our efforts on gun control,
but the most powerful key will come
when we are able to grasp what has been going on
in the mind of the shooter
that has set him on the path toward murder/suicide
and we find ways to prevent,
or detect and alter,
that state of mind.